The spine is one of the most vital parts of the human body. Made up of hard, sturdy vertebrae that enclose the spinal cord, this structure not only supports the body, but also encases the nerves that allow the brain and body to communicate so that the body may function.
Quadriplegia, also known as tetraplegia, is the paralysis of all four limbs of the body. Though quadriplegia may be caused by incidents such as stroke or meningitis, it is most commonly the result of a spinal cord injury (SCI).
An SCI is damage to the spinal cord or nerves at the end of the spinal canal that often causes permanent damage in body function, the severity of the damage dependent on where the injury takes place. Although the causes of SCI vary, such as violence and falls, the majority of SCIs are due to motor vehicle accidents.
Levels of Injury
The first eight vertebrae that make up the spine are called the cervical vertebrae. Abilities of the patient following SCI will vary depending on the location of the injury as well as factors such as age, weight and other existing medical conditions.
C1-C3 QUADRIPLEGIA
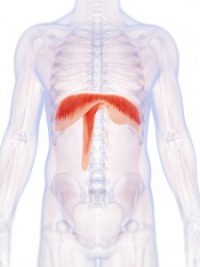
Injury within this region of the spine typically results in complete paralysis of the arms and legs, with limited neck movement depending on the muscle strength of the individual. A patient with this type of injury will have a compromised sympathetic nervous system and require complete care with everyday tasks, ranging from eating to domestic care of their household. In addition, the patient will be fully ventilator dependent, as the diaphragm muscles used to breathe will also be paralyzed.
C4 SPINAL CORD INJURY
Patients with a C4 injury will generally have full head and neck movement as well as slight shoulder movement, though there is still full paralysis of the arms and legs. As with the C1-C3 injury, complete care is usually still required. With regards to the respiratory system, the patient may be weaned from a mechanical ventilator, but assistance with coughing and removal of secretions may be necessary.
C5 SPINAL CORD INJURY
With injury to this vertebrae, there is typically full neck and head movement with good muscle strength as well as good shoulder control. There is still paralysis of the arms and legs at this level with varying degrees of elbow movement, but the individual may be able to feed themselves using a feeding strap and fork or spoon so long as the food is precut.
Patients with a C5 injury have more independence, as some may have the ability to drive a car fitted with special hand controls and complete small tasks with assistance such as loading their wheelchair into a car or brushing their hair by use of palm straps. Additionally, patients may breathe without ventilator assistance but may have low stamina and tire easily.
C6 SPINAL CORD INJURY
With a C6 injury, there is enough movement in the hands that an electric wheelchair with hand controls for uneven surfaces may be used as well as a manual wheelchair for a short period of time on a flat surface. Although precut food must still be eaten with a feeding strap, those with C6 injury may make themselves hot drinks with a special kettle apparatus.
Ventilator assistance is not necessary for this level of injury but clearing secretions and coughing still require help. Most patients also have the ability to dress the upper half of their body by themselves as well as perform simple grooming tasks such as shaving and brushing hair and teeth with the use of palm straps.
C7- C8 SPINAL CORD INJURY
The lowest part of this section of the spine, injuries on this level allow for more significant movement and independence depending on flexibility and strength of the individual. Self-feeding, prolonged electric wheelchair use and bladder/bowl manageability are all possible at this point. In addition, showering of the upper body, grooming and making small meals are also possible. Mechanical ventilation is not needed for this level of injury, but the patient may experience low stamina.
Those with a spinal injury below the cervical spine are paraplegic, with full function of the upper extremities and full control of the respiratory system.
The Avery Diaphragm Pacing System System
For those with an injury sustained above C5 and currently on a ventilator, the Avery Diaphragm Pacing System may be considered for qualified candidates as an alternative to mechanical ventilation.
The Avery Diaphragm Pacing System is designated for quadriplegic patients who are ventilator dependent due to residual function of their diaphragm, lungs, and phrenic nerves. By surgically implanting an electrode beside the phrenic nerve, the device sends electrical impulses in order to restore function to the diaphragm.
Compared with a mechanical ventilator, patients typically prefer the Avery Diaphragm Pacing System. When the Diaphragm Pacing System stimulates the diaphragm via the phrenic nerve and draws air into the lungs (negative pressure), it is more physiologically accurate as well as more comfortable for the patient.
With mechanical ventilation, air is forced into the lungs (positive pressure) which is an unnatural action for the body and may cause physical distress. Additionally, patients using a mechanical ventilator are at risk for ventilator-associated pneumonia and other upper airway infections.
The Story of Andrea
Following a motor vehicle accident in September 1990, Andrea became a C1-C2 quadriplegic and was placed on a mechanical ventilator. Then, in April 1991, she was implanted with a diaphragm pacing system and has been pacing 12-14 hours a day since.
As a result of the implantation of her pacers, Andrea had the freedom to attend college, receiving both her bachelors as well as her master’s degree. She now works as a mental health counselor, and credits the dramatic change in her life to her Avery pacemaker.